PCOS is under-researched relative to its prevalence, which creates genuine knowledge and training gaps among healthcare providers. It’s also a complex, multisystem condition that rarely follows a textbook presentation, making diagnosis feel arbitrary and the path forward unclear.
Many of my patients arrive carrying that same frustration, alongside a tangle of unanswered questions, such as:
- ‘Do I actually have cysts?’
- ‘Why are my symptoms so different from what I’ve read online?’
- ‘Why has no one explained how all of this fits together?’
If any of this sounds familiar, know that your confusion is not a reflection of you – it reflects a system that hasn’t yet caught up with the complexity of this condition. But that is changing.
In 2026, after years of research and global collaboration, PCOS was officially renamed PMOS (polyendocrine metabolic ovarian syndrome). And while that may sound like a simple change in terminology, it represents something far more significant – a long-overdue shift in how this condition is understood and how people living with it are cared for.
Why did the name need to change?
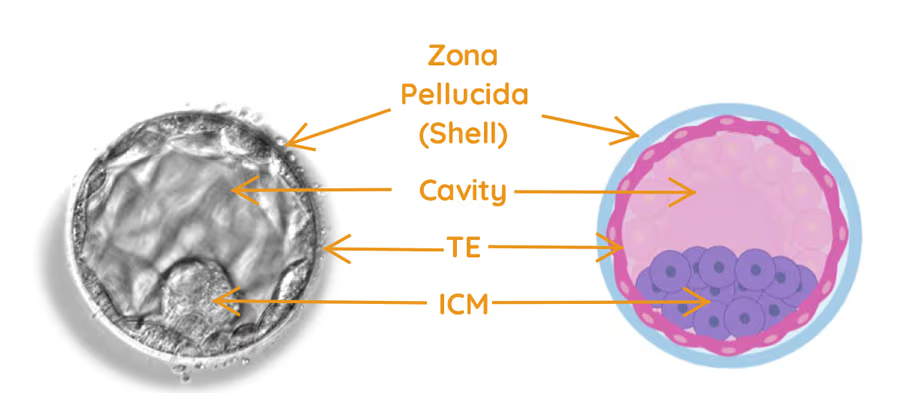
The term ‘polycystic ovary syndrome’ has always been misleading. It implies the condition is defined by cysts on the ovaries, but many people with this diagnosis don’t have ovarian cysts at all. What appear as ‘cysts’ on ultrasound are often immature follicles – not true cysts in the clinical sense.
More importantly, PMOS is not just an ovarian condition. What we now understand is that it’s a complex hormonal and metabolic syndrome affecting multiple systems throughout the body, extending well beyond the reproductive organs.
The old name unintentionally narrowed the focus to the ovaries, and patients paid the price with delayed or no diagnoses. In fact, it’s estimated that up to 70% of people with this condition don’t know they have it.1 Symptoms beyond the reproductive system, such as weight changes, insulin resistance and mood disturbances, were routinely overlooked. Some people were told they didn’t have the condition simply because their ultrasound looked normal.
This renaming isn’t cosmetic. It’s a correction of decades of misunderstanding. And for many, it will mean the difference between feeling dismissed or properly seen by your healthcare practitioner.
What PMOS actually means
PMOS may sound like a more complex term, but it is far more accurate. The new name reflects three interconnected aspects of the condition:
- Polyendocrine – multiple hormonal systems are involved, not just the ovaries
- Metabolic – the condition affects how your body regulates insulin, energy and weight
- Ovarian – ovulation and reproductive function remain part of the picture.
Put simply, PMOS recognises that your symptoms are connected, not random. Irregular cycles, acne, excess hair growth, difficulty losing weight, mood changes and fertility challenges are not separate, unrelated problems. Rather, they are different expressions of the same underlying hormonal disruption.
And importantly, this is a condition we understand and manage far better today than ever before.
What this means for you
For many people, this change validates what they have felt all along – that their symptoms are real, that they are connected, and that they deserve more than piecemeal care.
You may also find that conversations with your healthcare team are approached differently. Rather than focusing primarily on your menstrual cycle or the appearance of your ovaries on ultrasound, there is likely to be greater emphasis on hormone balance, metabolic health (particularly insulin resistance) and long-term wellbeing, including cardiovascular risk and mental health.
This holistic approach is exactly what many patients have been asking for.
A question I’m often asked: ‘Will my menstrual cycle become regular again?’
In many cases, the answer is yes.
PMOS often disrupts ovulation through a combination of hormonal imbalance and insulin resistance. When we address these underlying drivers, we frequently see menstrual cycles becoming more regular, ovulation returning and symptoms improving more broadly.
That said, there is no quick fix. For most patients, meaningful and lasting improvement comes from consistent, sustainable changes built up over time – not from any single intervention.
Lifestyle as medicine
Lifestyle changes are the first-line treatment for PMOS because they directly target the two core drivers of the condition – insulin resistance and hormone dysregulation.
This doesn’t mean extremes or perfection. It means:
- Nourishing your body with foods that stabilise blood sugar
- Moving regularly in a way that feels sustainable, not punishing
- Prioritising sleep and managing stress.
Even small, consistent shifts can have a meaningful impact on ovulation and menstrual cycle regularity.
When lifestyle changes aren’t enough
For some people, lifestyle changes alone won’t fully address their symptoms. This is a reflection of the condition’s complexity, not a personal failing.
Depending on your symptoms and goals, we may consider:
- Hormonal treatments to regulate the menstrual cycle and reduce the effects of elevated androgens (responsible for symptoms like acne and excess hair growth)
- Medications, such as metformin, to support insulin function and metabolic health
- Ovulation induction if you’re trying to conceive a baby.
These aren’t a sign of failure or of doing something wrong. They are simply additional tools – ones that work best when built on the foundation of the lifestyle changes already discussed.
Looking after the whole of you
One of the most important shifts that comes with the PMOS reframing is that your care should extend beyond physical symptoms alone. This condition doesn’t just affect your ovaries – it affects how you feel in your body every day, and your care should reflect that.
The mental and emotional toll of living with a complex diagnosis, sometimes compounded by years of feeling unheard, deserves the same attention as your physical symptoms. So too does the impact that visible symptoms, such as acne, hair changes and weight shifts, can have on body image and self-esteem. Equally important is monitoring the long-term health risks associated with PMOS, particularly an elevated risk of type 2 diabetes and cardiovascular disease – both of which are very manageable with the right support.
What this means if you’ve been living with PMOS
If you’ve struggled with a confusing or inaccurate diagnosis, this new name is significant as it represents a fundamental shift in how the condition is understood, not just what it’s called.
Your symptoms are not random, your experience is valid, and your care should be as individual as you are.
At Newlife IVF, we approach PMOS not as a label to manage, but as an opportunity to truly understand your body and build a path forward that feels achievable.
So if you’re living with PMOS and would like expert advice about ways to improve your chances of getting pregnant, you can make an appointment with one of our fertility specialists by calling Newlife IVF on (03) 8080 8933 or by booking online via our appointments page.
Reference
- World Health Organisation [Internet]. Polycystic ovary syndrome. Jan 2026 [cited 2026 2 June]. Available from: https://www.who.int/news-room/fact-sheets/detail/polycystic-ovary-syndrome