Here, we break down what embryo grading really represents, how it is used in IVF laboratories, and what it means – and does not mean – for your chances of success.
What is embryo grading?
Embryo grading is a system embryologists use to describe the appearance of an embryo under the microscope at a specific moment in time. It allows us to make informed decisions about which embryos to transfer or freeze, and to communicate clearly within the laboratory team when assessing embryo development.
Importantly, embryo grading is a descriptive tool rather than a guarantee of outcome. IVF laboratories may use slightly different grading systems, which means embryo grades can vary between clinics – even clinics located within the same state – and are not always directly comparable. Understanding what grading does and does not tell us can help you feel more informed and reassured throughout your IVF journey.
Why is so much attention given to embryo grading?
It’s natural to want something tangible to hold onto during IVF, and embryo grades can feel like a clear point of reference. Much like our early educational experiences, receiving a ‘grade’ can feel like an assessment of performance. Many people assume that a higher grade means a better embryo (and therefore a higher chance of success), while a lower grade suggests the opposite.
While this interpretation is understandable, it isn’t entirely accurate. There are many factors involved in embryo development and implantation, and grading alone cannot capture them all.
Embryo grading is not a prediction tool; it is an observation tool. It tells us what an embryo looks like at a particular point in time, not whether it will implant or result in a pregnancy. Every viable embryo, regardless of grade, has the potential to result in a pregnancy.
In our many years of experience in IVF laboratories, we have seen high-grade embryos that did not implant, and lower-grade embryos that went on to become healthy babies. While grading helps us prioritise embryos for transfer or freezing at that moment, it is only one piece of a much larger picture.
When do we grade embryos?
Embryos are grown in the Newlife IVF laboratory for up to six days after fertilisation. By day five or six, embryos ideally reach the blastocyst stage, which marks a critical milestone in development.
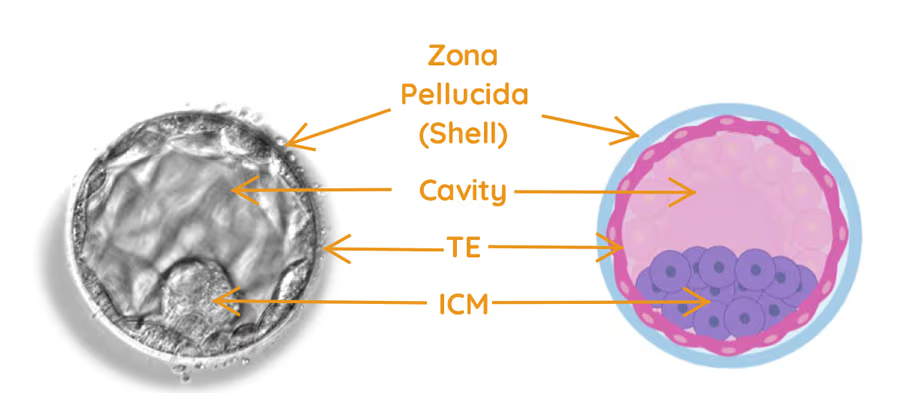
At this stage, the embryo has developed into many interacting cells, and for the first time, we can clearly identify three distinct structures:
- Inner cell mass (ICM): A cluster of cells inside the embryo that will eventually form the baby
- Trophectoderm (TE): The outer layer of cells that will develop into the placenta, which supports the baby during pregnancy
- Blastocoel: A fluid-filled cavity that allows the embryo to expand.
How does blastocyst grading work?
Blastocyst grading assesses three main features: the stage of expansion, the characteristics of the inner cell mass, and the characteristics of the trophectoderm. Each component is graded separately, as outlined below.
Expansion stage
The expansion stage refers to the size of the blastocyst and how far it has progressed in breaking free from its protective outer shell, known as the zona pellucida. As the blastocyst grows, it needs to thin and eventually break through this shell in a process called hatching.
Expansion is categorised into six stages:
- Stage 1: Early blastocyst development, where a small fluid cavity is just beginning to form
- Stage 2: Early expanding blastocyst, with a growing cavity but still relatively small within the shell
- Stage 3: Expanded blastocyst, where the cavity is larger and the embryo occupies more space, but hatching has not yet begun
- Stage 4: Fully expanded blastocyst, filling most of the shell, which has thinned significantly
- Stage 5: Beginning to hatch, with part of the embryo emerging through the shell
- Stage 6: Fully hatched, where the embryo has completely escaped the zona pellucida and is ready for implantation.
Inner cell mass (ICM) characteristics (A–D)
The inner cell mass is the group of cells that will go on to form the baby. It is graded from A to D based on appearance:
- A: Many healthy cells that are tightly packed
- B: Several cells with a slightly looser arrangement
- C: Few cells that are scattered and less cohesive
- D: Very few or degenerating cells (considered non-viable).
Trophectoderm characteristics (A–D)
The trophectoderm forms the placenta and is also graded from A to D:
- A: Many cells are present, forming a strong and cohesive layer
- B: A moderate number of cells with less uniformity
- C: Few cells with an irregular appearance
- D: Very few or degenerating cells (considered non-viable).
Putting it all together
When you see an embryo grade, it is simply a shorthand way of combining these three observations into a single description.
For example, a grade of 5AB means:
- 5: The blastocyst is beginning to hatch from its outer shell
- A: The inner cell mass has many tightly arranged cells
- B: The trophectoderm has a reasonable number of cells forming a mostly cohesive layer (although the layer may not be uniform).
While this grading helps embryologists make informed decisions in the laboratory regarding embryo quality, it’s important to remember that no single grade can determine the outcome of an embryo.
Embryo grades are not fixed and can change over time
Embryo grading provides a snapshot in time. Embryos are dynamic and continue to grow, divide and change as they develop.
For example, an embryo graded early on day five as 2CB may look quite different later the same day, potentially developing into a 4BB embryo. This progression is entirely normal and reflects ongoing development in a viable embryo.
The same principle applies when an embryo is transferred, while others continue developing in the laboratory. An embryo transferred on day five may be graded 3BB, while its siblings reassessed later could receive a seemingly higher grade, like 5AA. This difference is often due simply to timing and additional hours of development – not because the transferred embryo was a poorer option.
At the time of transfer, the chosen embryo was assessed as the best option based on its developmental stage, appearance and timing. Because grading is so closely linked to when an embryo is observed, it is not a reliable way of comparing embryos with one another. Instead, grading is just one part of a broader decision-making process.
You can learn more about this approach in our blog, How we select embryos for transfer.
What grading can (and can’t) tell us
In general, higher embryo grades are associated with higher pregnancy rates, which is why grading remains a useful tool when deciding which embryos to transfer or freeze.
However, embryo grading is not an absolute predictor of outcome. A high-grade embryo does not guarantee a pregnancy, and a lower-grade embryo does not mean a pregnancy will not occur. In practice, we regularly see examples where a high-grade embryo, such as 6AA, does not implant, while a sibling embryo with a lower grade goes on to result in a healthy baby.
Once a pregnancy is established, the embryo’s grade is no longer relevant. It does not predict whether a pregnancy will continue, nor does it reflect the future health of the baby.
If an embryo has been transferred or frozen, it has been deemed viable and has potential. Every viable embryo, regardless of grade, has the capacity to become a baby. For patients with embryos of varying grades in storage, or those who have had a lower-grade embryo transferred, there is every reason to remain hopeful.
Looking beyond letters and numbers
Embryo grading is only one part of how we assess embryo development. In addition to visual grading, we use time-lapse imaging, key developmental milestones, embryologist expertise and AI-powered tools to observe how embryos grow and behave over time.
Together, these approaches provide a better understanding of embryo health and potential, helping us make the most informed decisions for your treatment.
Our guidance for patients
We encourage Newlife IVF patients to focus on the number of viable blastocysts rather than becoming fixated on letters and numbers. An embryo’s potential is far greater than its grade alone.
If an embryologist has transferred or frozen your embryo, the embryo has the capacity to continue developing, and this potential matters far more than a single snapshot assessment.
Interested to learn more about embryo grading or IVF?
If you would like to understand more about embryo grading or IVF treatment, be sure to listen to the embryo optimisation podcast episode. Our team at Newlife IVF is also here to support and guide you throughout your fertility journey – call us on (03) 8080 8933.
